For higher degrees of myopia (typically approximately −7 dioptres or more), corneal laser procedures are often no longer suitable. In these cases, visual acuity can be significantly improved through lens-based surgery. In principle, two procedures are available.
Treatment of high myopia without laser
Phakic intraocular lens (ICL)
Patients with high myopia are often no longer suitable candidates for common laser procedures such as LASIK or SMILE. In such cases — typically from about −7 dioptres or more — implantation of a phakic intraocular lens may be considered, usually an ICL (implantable collamer lens). In this procedure, an artificial lens is implanted in addition to the natural lens without removing it.
Prof. Findl predominantly uses the ICL, which is positioned behind the pupil and iris. The lens consists of a very thin, soft material and is implanted through a small corneal incision. The procedure is performed as an outpatient day-case procedure under local anaesthesia.
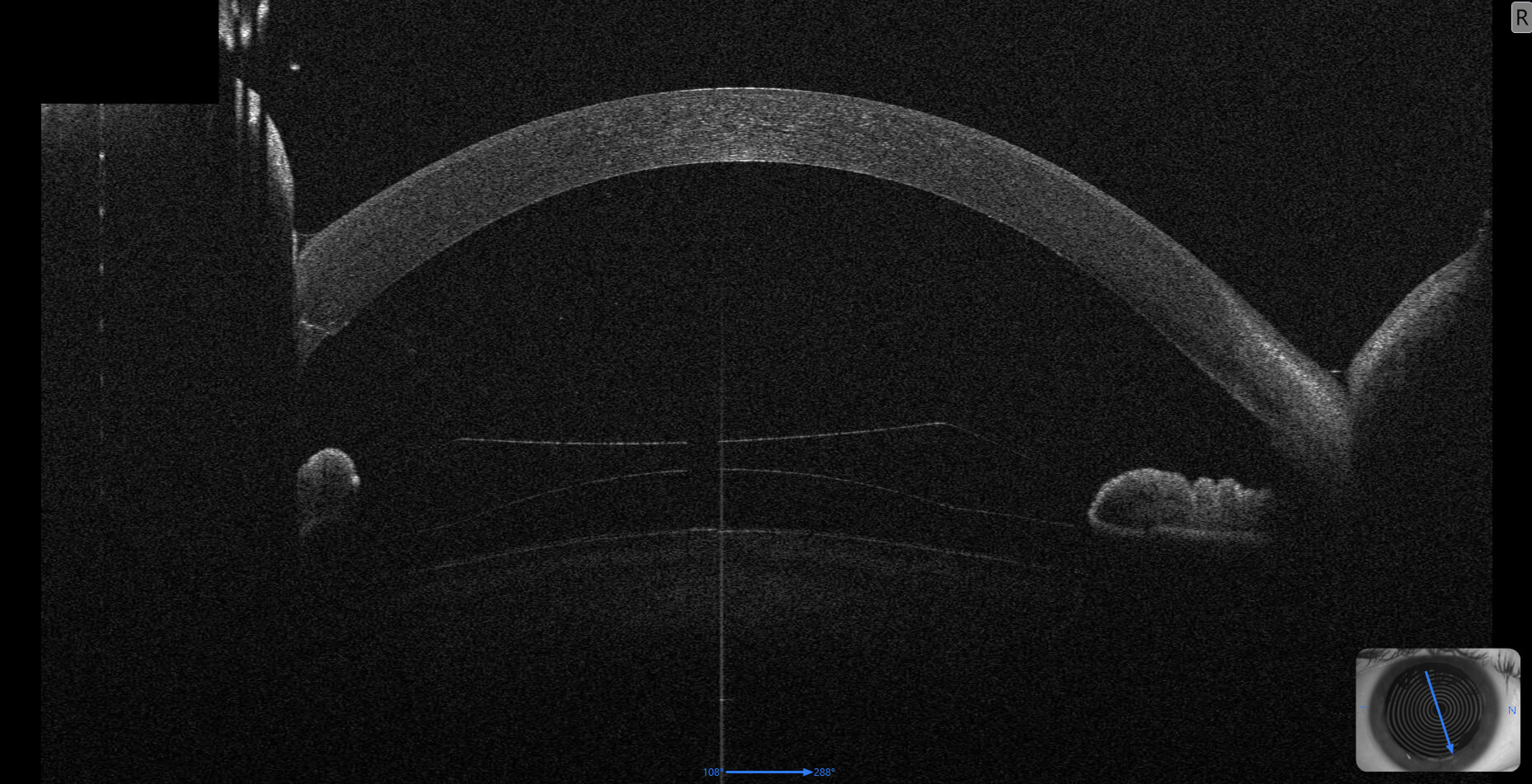
A particular challenge is accurate sizing of the lens diameter, as it must precisely match the individual anatomy of the eye. Therefore, several highly precise measurements are performed preoperatively using two different modern anterior segment OCT devices. Using new, partly AI-supported algorithms, lens size can be determined more accurately than with the manufacturer’s standard method.
Additionally, suitability of the eye for this surgery is carefully evaluated — including endothelial cell imaging, which is also performed in Prof. Findl’s practice.
The ICL is often the preferred alternative to refractive lens exchange, especially in younger patients, because the natural lens remains intact. Which method is safest and most appropriate long-term is decided individually after complete diagnostics.
Refractive lens exchange (Clear Lens Exchange / RLE)
Alternatively — similar to cataract surgery without cataract — the natural lens can be removed and replaced with an intraocular lens. This usually allows the refractive error to be fully corrected.
However, in myopic eyes there is a relevant risk of retinal detachment. The decisive factor is the status of the vitreous body before surgery. An international ESCRS-supported multicentre study led by Prof. Findl (MYOPRED multicentre study) in more than 900 eyes demonstrated for the first time that if a complete posterior vitreous detachment is not present before surgery, the risk of retinal detachment after such lens surgery is approximately six- to seven-fold higher.
Therefore, a specialised OCT examination is performed before surgery to assess the vitreous status precisely.
Frequently asked questions about phakic intraocular lenses (ICL)
Who is a phakic intraocular lens suitable for?
An ICL is mainly suitable for patients with high myopia for whom laser procedures such as LASIK or SMILE are not (or no longer) appropriate — typically from about −7 dioptres or more. Whether an ICL is suitable in an individual case is determined after detailed examination by Prof. Findl.
What is an ICL (implantable contact lens)?
The ICL is a phakic intraocular lens inserted in addition to the natural lens. The natural lens remains completely intact. Prof. Findl positions the lens behind the iris, and it is not visible from the outside.
How is ICL surgery performed?
The procedure is performed as an outpatient day-case surgery under local anaesthesia. The lens is inserted through a small corneal incision. The operation usually takes only a short time and is well tolerated by most patients.
Why is accurate ICL sizing so important?
The ICL diameter must precisely match the anatomy of the eye. Accurate calculation is crucial for safety and long-term outcome. Therefore multiple high-precision measurements using modern anterior segment OCT devices are performed. Prof. Findl also uses new partly AI-supported algorithms that provide more accurate calculation than the manufacturer’s standard method.
Which examinations are necessary before ICL implantation?
In addition to anterior segment OCT measurements, endothelial cell imaging is performed to determine whether the cornea is suitable for a phakic lens. These examinations are performed in Prof. Findl’s practice.
What are the advantages of refractive lens exchange (RLE)?
Even high refractive errors can usually be fully corrected. Age-related presbyopia can also be treated simultaneously using specialised intraocular lenses. Prof. Findl advises individually which lens type is most suitable.
What are the risks of refractive lens exchange?
In myopic eyes there is an increased risk of retinal detachment. A decisive factor is the vitreous status: if a complete posterior vitreous detachment is not present before surgery, the risk increases. Prof. Findl evaluates this using specialised OCT examination and carefully assesses suitability.